
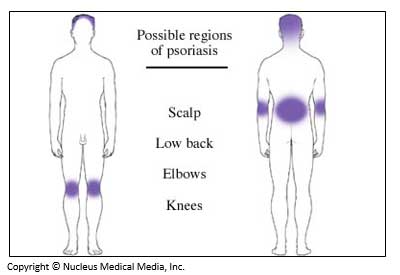
Psoriasis is a chronic, noncontagious skin condition characterized by scaling and inflammation. The inflamed skin forms red, thickened areas with silvery scales. The condition is most commonly found on the scalp, elbows, forearms, knees, shins, ankles, and lower back. It also may affect the fingernails, toenails, and soft tissues of the mouth, genitals, and joints. The inflamed skin can cause pain and discomfort from cracking, but psoriasis is rarely itchy.
Possible Regions of Psoriasis
Types of Psoriasis
Plaque Psoriasis—This is the most common form. It is characterized by raised lesions that have a reddened base covered by silvery-white scales. The scales shed frequently and are very dry.
Guttate Psoriasis—This type is often triggered by bacterial infections like strep throat and is most common in young adults and children. It is characterized by small, salmon pink, drop-like lesions on the trunk, limbs, and scalp. It may clear up on its own after a few weeks or months.
Pustular Psoriasis—Blisters of non-infectious pus appear on the skin and may affect small or large areas of the body, most commonly fingers, palms and soles. This type of psoriasis usually is triggered by medications, infections, emotional stress, or certain chemicals.
Inverse Psoriasis (also called flexural or intertriginous psoriasis)—This type is usually found in skin fold areas, such as the armpits, under the breasts, or near the genitals or buttocks. It is more common in people who are overweight and may be exacerbated by friction or sweating in skin fold areas. The plaques are red, smooth, dry and large.
Erythrodermic Psoriasis—This is the least common form of psoriasis and is characterized by widespread reddening and scaling of the skin as well as severe itching and skin discomfort. This form occurs after a severe sunburn or use of certain medications.
Some people with psoriasis also develop a condition called psoriatic arthritis. This occurs when the inflamed areas of the skin are accompanied by joint inflammation, most often in the hip, spine, knee, or elbow joints. In some cases, psoriasis severely compromises quality of life. In addition to physical discomfort, people with psoriasis may develop emotional problems, such as depression or anxiety, and may experience social difficulties due to visible plaques. If you or a family member is suffering from psoriasis, seek out counseling, support groups, and services.
Causes of Psoriasis
The exact cause of psoriasis is unknown, but some theories suggest that it may be a disorder of the immune system. T-cells, a type of white blood cell that normally protects the body against infection, can trigger inflammation and excessive skin cell reproduction that cause skin to shed too rapidly. Psoriasis flare-ups may be due to a variety of factors, including environment, certain medications, and stress.
Plaque psoriasis first appears during two peak age ranges. The first peak occurs in persons aged 16-22 years, and the second occurs in persons aged 57-60 years. It is considered quite rare in infants, but may occur in children before the age of 10. Psoriasis is more prevalent in fair-skinned people, especially those who have a blood relative with psoriasis. It is less common in people with darker skin. Psoriasis is often triggered by weather conditions. In general, people living in cold, dry climates are at much greater risk of developing psoriasis than people living in temperate or warm climates. In fact, warm, humid weather helps to heal psoriasis symptoms.
Risk Factors
It is possible to develop psoriasis with or without the risk factors listed below. In fact, most cases of psoriasis are not associated with any of the risk factors listed below. However, the more risk factors you have, the greater your likelihood of developing psoriasis. If you have a number of risk factors, ask your doctor what you can do to reduce your risk. Risk factors include:
Genetics—There is a strong genetic component to psoriasis. In about one-third of all cases, there is a family history of psoriasis.
Medical Conditions—conditions that are most likely to trigger psoriasis include:
- Stress/emotional disorders—Stress, suppressed anger, anxiety, depression, or other emotional disorders can trigger psoriasis outbreaks.
- Infection—Psoriasis frequently flares up after upper respiratory infections like tonsillitis, sinusitis, or strep throat.
- Skin injuries—Psoriasis may develop at the site of a previous skin injury or mild abrasion, such as a cut, burn, or injection. Delayed development of psoriasis at these injured skin sites is known as the Köbner Phenomenon.
- HIV/AIDS—Psoriasis may become particularly severe in people infected with HIV/AIDS.
- Obesity—There is some evidence that obesity exacerbates psoriasis.
- Alcoholism—It is not entirely clear whether alcoholism is a risk factor for developing psoriasis, but consuming excessive amounts of alcohol should be discouraged, especially during periods of psoriasis flare-ups.
Medications—Certain medications have been associated with triggering or exacerbating outbreaks of psoriasis. These include:
- Beta-blocker and angiotensin-converting enzyme (ACE) inhibitors—used to treat high blood pressure
- Lithium—Used to treat severe depression or bipolar disorder
- Hydroxychloroquine and Chloroquine—used to prevent malaria
- Non-steroidal anti-inflammatory drugs (NSAIDs)—Certain types of NSAIDs may cause or worsen psoriasis; however, other types of NSAIDs may actually improve psoriatic symptoms.
Treatment Options
Treatment is based on the severity of the disease, the extent and location of the areas involved, and responsiveness to the treatment. Options include:
Topical Treatment
Many patients respond well to treatments applied directly to the skin. Topical treatments include:
- Corticosteroid creams and ointments (most common treatment)
- Synthetic forms of vitamin D and retinoids
- Retinoids
- Coal tar preparations
- Bath solutions and moisturizers
- Tacrolimus and pimecrolimus (especially for inverse psoriasis)
Photo (Light) Therapy
If psoriasis covers more than 30% of the body, it is difficult to treat with topical medications alone. Daily, short, non-burning exposure to sunlight clears or improves psoriasis in many people. Sunlight is often included among initial treatments. A more controlled form of artificial light treatment (UVB phototherapy) is used in cases that are more widespread. Alternatively, psoriasis can be treated with ultraviolet A (UVA light) and psoralen, a treatment known as PUVA. Psoralen is an oral or topical medication that makes the body more sensitive to light.
Phototherapy can be very effective in controlling psoriasis but it requires frequent treatments. It may cause side effects such as nausea, headache, and fatigue, burning, and itching. Both UVB and PUVA may increase the risk for squamous cell and melanoma skin cancers.
Systemic Treatment
For more severe types of psoriasis, doctors may prescribe a number of other powerful medications, which can be effective, but are associated with side effects that are more serious. These include:
- Methotrexate—a type of systemic medication that affects the whole immune system; should not be taken by pregnant women, women planning to become pregnant, or by their male partners
- Cyclosporine—another type of systemic medication that suppresses the immune system to slow the turnover of skin cells; should not be taken by pregnant or breastfeeding women
- Hydroxyurea—less toxic than methotrexate or cyclosporine, but may be less effective
- Systemic retinoids—Compounds with vitamin A-like properties taken internally may be prescribed in severe cases. Retinoids can cause birth defects, and women must protect themselves from pregnancy for several years after completing treatment. Systemic retinoids are often combined with phototherapy for increased effectiveness and for their property of being protective against squamous skin cancer.
- Newer medications include biologic agents, which affect a part of the body's immune response by targeting certain cells in the immune system that cause inflammation.